

By MATTHEW HOLT
If well being coverage wonks consider something it’s that major care is an efficient factor. In principle we should always all have robust relationships with our major care docs. They need to navigate us across the well being system and be arriving on our doorsteps like Marcus Welby MD when wanted. Wonks like me consider that in the event you introduce such a relationship sufferers will obtain preventative care, will get on the fitting meds and take them, will keep away from the emergency room, and have fewer hospital admissions—in addition to costing an entire lot much less. That’s in massive the speculation behind HMOs and their latter-day descendants, value-based care and ACOs
In fact there are first rate examples of major care-based methods just like the UK NHS and even Kaiser Permanente or the Alaskan Artic Slope Native Well being Affiliation. However for many People that’s fantasy land. As a substitute, we have now a system the place major care is the ugly stepchild. It’s being slowly throttled and picked aside. Even the wealth of Walmart couldn’t make it work.
There are at the least 3 forms of major care which have emerged over current a long time. And none of them are actually profitable in making that “major care because the lynchpin of inhabitants well being” concept work.
The primary is the first care physician bought by and/or working for the massive system. The purpose of those practices is to be sure that referrals for the costly stuff go into the proper hospital system. For a very long time these major care docs have been shedding their employers cash—Bob Kocher said $150-250k a year per doctor in the late 2000s. So why are they saved round by the larger methods? As a result of the sufferers that they do admit to the hospital are insanely worthwhile. Contemplate this NC system which ended up suing the big hospital system Atrium as a result of they solely needed the referrals. As you may anticipate the “value saving” advantages of major care are robust to search out amongst these methods. (In case you have time watch Eric Bricker’s video on Atrium & Troyon/Mecklenberg)
The second is pressing care. Pressing care has changed major care in a lot of America. The number of urgent care centers doubled in the last decade or so. Whereas it has taken some strain off emergency rooms, Pressing care has changed major care as a result of it’s handy and you’ll simply get appointments. However it’s not doing inhabitants well being and care administration. And sometimes the pressing care facilities are owned both by hospital methods which might be utilizing them to generate referrals, or non-public fairness pirates which might be attempting to spice up prices not management them.
Thirdly telehealth, particularly hooked up to pharmacies, has enabled a lot of folks to get entry to drugs in a less expensive and extra handy vogue. In fact, this isn’t actually full major care however HIMS & HERS and their many, many rivals are enabling entry to frequent antibiotics for UTIs, contraceptive drugs, and in addition psychological well being drugs, in addition to these boner and baldness drugs.
That’s to not say that there haven’t been makes an attempt to construct new forms of major care
Oak Avenue, ChenMed and Iora (now a part of One Medical) had been constructed with the thought of bumping up the first care providers given to seniors in Medicare Benefit, with the concept that–like Kaiser and its rivals–they will take monetary danger for specialty and hospital care. The speculation, as Iora’s founder Rushika Fernandopulle all the time stated, was “double the spending on major care and scale back general prices by 30%.” It’s not too clear in the event that they ever bought there.
In fact like every little thing else in American well being care Oak Avenue and Iora had been repeats of earlier efforts by Mullikin, Pleasant Hills, HealthPartners and plenty of extra to handle general care prices by taking major care capitated danger. None of those experiments had been left alone by the finance bros lengthy sufficient to see what would have occurred in the event that they performed out. The inventory market of the Nineties and the 2020s are filled with graveyards of publicly traded major care teams that each one had very promising begins. Had they been left alone lengthy sufficient to develop organically it’s potential that we might see a special future. We would even see that future if Included Well being, Transcarent and others handle to construct out their major care/telehealth/navigation/Facilities of Excellence providing. However it’s going to take some time
General, risk-bearing major care stays a lonely enterprise regardless of it being the popular coverage wonk resolution since Sydney Garfield began taking prepayment from staff on the Grand Coulee Dam in 1933
In fact this being America you possibly can nonetheless get wonderful major care, it’s simply going to value ya.
Silicon Valley multi-millionaires pay Jordan Shlain’s Private Medical $40k a 12 months plus for white glove service. On the different finish of the dimensions, One Medical collects $80-200 a 12 months from sufferers paying for entry to subsequent day appointments, NPs who truly reply emails and a free telehealth service for pressing care. In between is an entire host of docs who’ve opted out of the effort of billing insurers and are charging between $500 and $5000 a 12 months for concierge care. Then there are a ton of major care based mostly providers utilizing telehealth, dwelling visits and NPs, usually mixed with onsite clinics at workplaces
Which signifies that the variety of these offering real Marcus Welby MD fashion major care in the neighborhood continues to fall.
And it’s not too onerous to determine why. The typical major physician makes an entire lot lower than their specialty counterparts.
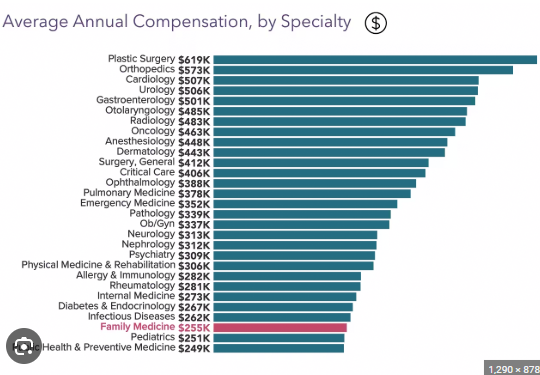
The charges for major care are low. They’re set that manner intentionally by the RUC (the Relative worth scale replace committee) which is dominated by specialists and essentially sets Medicare fees, that are then adopted by most non-public insurers. So most docs have a tendency to have a look at the highest finish of this chart slightly than the underside they’re selecting their residency slots. American well being care is dear as a result of we have now too many specialists doing marginally helpful care, and too many hospitals (and pharma and machine firms) making financial institution off them. And it’s all associated to that chart.
There was a slightly odd depend by KFF saying that nearly 50% of American doctors were in primary care, however that counted an entire lot of docs are “major care” who don’t ship conventional major care. That is after all unsuitable but it surely provides a touch for the answer.
There are 340 million People. We may give everybody a PCP and put them in a panel of 600 folks (versus the 2-3,000 typical PCP panel. That quantity occurs to be what MDVIP and other concierge services offer. That might require 570 thousand PCPs. Which is about 60% of docs post-residency in America.
So if we transformed all these at the moment licensed PCPs and added NPs, we may give EVERYONE in America concierge fashion care. These docs could be instantly obtainable and assist their sufferers navigate the system.
Its proponents consider that concierge medication isn’t solely higher but additionally tends to be less expensive than common care. MDVIP claims that it saves $2500 per patient even after paying its docs extra, which is about 20% of well being spending. My competition is that we may give every PCP $2k per affected person (or $1.2m per 600 affected person panel), of which they may use (my guess) $300-500k to run their follow, they usually may preserve $700K to pay themselves.
So my proposal is we give everybody actually high-end major care, pay major care docs rather well and save a boatload of cash. And apparently we have now almost sufficient major care docs to do it. For certain in the event that they had been paid $700K a 12 months we’d quickly discover loads extra of them.
Matthew Holt is the Writer of THCB